


Africa’s demographic dividend: Delivering the promise in the context of a double disease burden
Authors
Share
There is no doubt: Africa will dominate global population dynamics in the 21st century. While public attention has long focused on Asia as a fast-growing and prospering market with currently 4.5 billion inhabitants, today’s one billion sub-Saharan Africans have significantly outpaced Asia in terms of population growth (2.6% vs. 1.1% in 2016, respectively).
The main reason for this ongoing population growth in sub-Saharan Africa (SSA) is a sharp decline in infant and child mortality whilst at the same time, continually high birth rates over the last few decades (the fertility rate per woman was 5.1 in 2013 compared to 6.7 in 1970, while infant mortality declined rapidly from 138 deaths per thousand births in 1970 to 67 in 2013). Today, one billion people or 16% of the world population live in SSA. By 2050, this number will double and in 2100, 3.9 billion people or 39% of the world‘s population could live in the region. This is the official forecast according to the Medium variant of the 2015 United Nations Population Projections.
A key condition today to fulfilling this demographic dividend (DD) is the formulation of policies that will help Africa to replicate the conditions that enabled East Asian countries to prosper during the period covering the early 1960s to the 1990s. The DD is defined as an accelerated economic growth triggered by the decline in a country’s birth and death rates and the relative increase in working-age adults. However, to open this demographic window of opportunity, public policies will in particular need to manage a rapid and significant decline in fertility in order to reduce the number of young dependents.
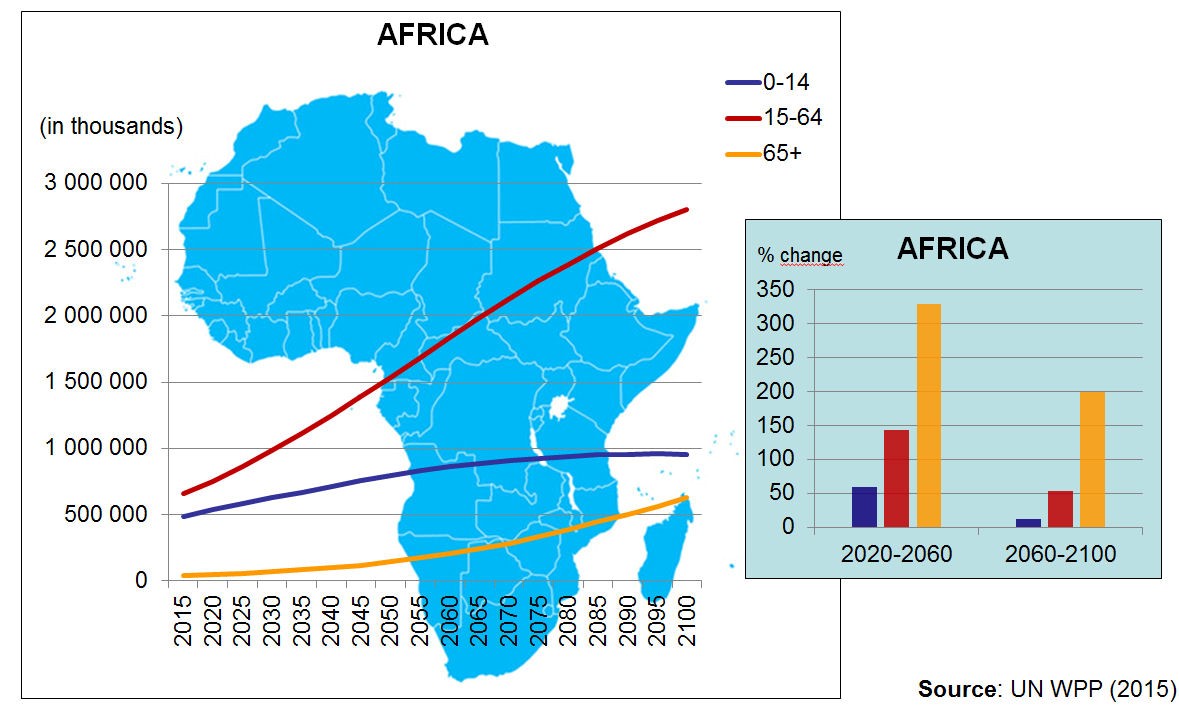
Population Growth in Africa 2015-2100 by Age Cohorts (World Demographic & Ageing Forum, 2016)
In addition, other topics are critical to capture this one-time opportunity in a sustainable manner:
Africans urgently need jobs. There will be no demographic dividend without new jobs. According to the International Monetary Fund (IMF), 18 million new jobs are needed every year till 2050. For just one year, this is equivalent to jobs for the entire population of the Netherlands. From now until 2050, the total number of new jobs required are almost equivalent to the entire European population.
Africa needs continued health investment and improvement. The window of opportunity for a demographic dividend only appears when fertility declines significantly and rapidly. This depends on further improvements of women’s and children’s rights and health outcomes. Making sure that women meet their reproductive health needs is a key priority. According to UNFPA, “countries with the greatest demographic opportunity for development are those entering a period in which the working-age population has good health, quality education, decent employment and a lower proportion of young dependents. Smaller numbers of children per household generally lead to larger investments per child, more freedom for women to enter the formal workforce and more household savings for old age. When this happens, the national economic payoff can be substantial”, and the demographic dividend delivers its potential.
It is clear that the demographic dividend will only become a reality if African countries invest into the health of their populations. Many countries have very successfully addressed the challenge of infectious diseases. An estimated three million children under age five have been saved from malaria and the incidence of new HIV cases in Sub Saharan Africa has fallen by more than half between 2001 and 2012. The next challenge is the rising epidemic of non-communicable diseases that also significantly affects this part of the world. It is too early to predict whether the success in the infectious disease area will repeat itself in the domain of non-communicable diseases. There are many obstacles to overcome. The countries of SSA have to integrate the policies to fight infectious diseases with those on NCDs, and to align the funding into one to avoid competition in resource allocation between the two areas. They need to develop integrated strategies that begin in the primary health care sector and finally, they need to define strategies on how to engage constructively with the private sector. There is much to consider.
 Universal and equal access to health care is an essential global challenge for the wellbeing of the world’s population and therefore requires the appropriate investment. The Lancet recently launched “The path to longer and healthier lives for all Africans by 2030: the Lancet Commission on the future of health in sub-Saharan Africa[1]”. The Commission highlights the importance of advocating an approach based on people-centred health systems which can be adapted to countries’ specific needs. Better health will not only benefit countries’ populations directly – it will also act as a catalyst, enabling the successful pursuit of other development agendas, as summarized in the Sustainable Development Goals (SDGs). As recommended in the Lancet article, a systemic and holistic approach is required, as “a fragmented health agenda will deliver some results but will not succeed in strengthening health service delivery and public health systems, and will not address the determinants of health“. Broad partnerships beyond the medical and health community are essential to move the health agenda forward.
Universal and equal access to health care is an essential global challenge for the wellbeing of the world’s population and therefore requires the appropriate investment. The Lancet recently launched “The path to longer and healthier lives for all Africans by 2030: the Lancet Commission on the future of health in sub-Saharan Africa[1]”. The Commission highlights the importance of advocating an approach based on people-centred health systems which can be adapted to countries’ specific needs. Better health will not only benefit countries’ populations directly – it will also act as a catalyst, enabling the successful pursuit of other development agendas, as summarized in the Sustainable Development Goals (SDGs). As recommended in the Lancet article, a systemic and holistic approach is required, as “a fragmented health agenda will deliver some results but will not succeed in strengthening health service delivery and public health systems, and will not address the determinants of health“. Broad partnerships beyond the medical and health community are essential to move the health agenda forward.
Failure is not an option. A bad outcome would challenge both Africa and the global community. Not succeeding in capturing a demographic dividend in Africa would lead to millions of people living in poverty and in slums. It would result in a restless young population and facilitate human suffering and social disruption that could spill over well beyond Africa. The implications for the globe as a whole must be considered, as today’s interconnected world shows that the issues and challenges that one continent faces will not be limited solely to one geographical area.
[1] http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(17)31509-X/fulltext
Authors


